The Vital Role of the Peroneal Muscles in Foot Function
The foot is composed of 26 bones, 33 joints and more than 100 muscles, tendons and ligaments.
It plays a role in propulsion, adapting to uneven ground, shock absorption and supporting body weight. It enables efficient movement and balance.
Co-ordination of the muscles and tendons within the foot and ankle is crucial for maintaining stability and adapting to variable terrains.
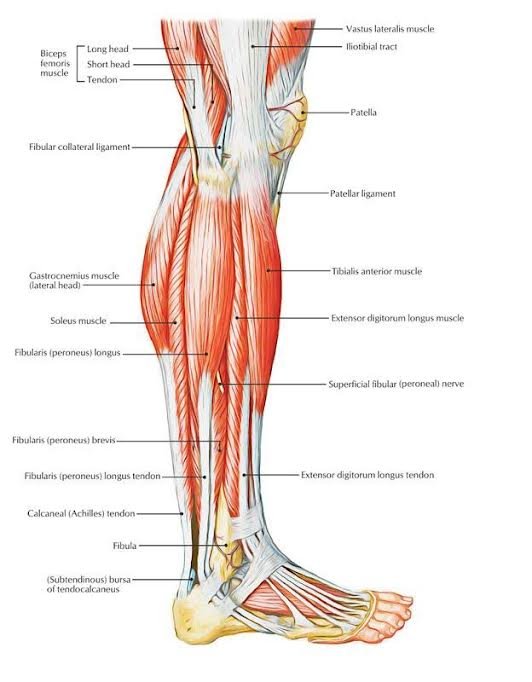
Among the key muscle groups contributing to foot biomechanics are the peroneal muscles. The peroneal complex is in the lateral compartment of the leg and extends across the ankle into the foot (see diagram below). It consists of:
Peroneus longus.
Peroneus brevis.
Peroneus tertius.
Accessory muscles: Quartus and Quintus
It is innervated by the superficial peroneal nerve (L5/S1) and supplied by the tibial and peroneal arteries.
Role of the Peroneal Muscles
Foot and ankle eversion (pointing outwards) and plantar flexion (pointing forwards).
Stabilisation of the first ray (first metatarsal and medial cuneiform on the inside of the foot).
Offloading the plantar fascia under the foot.
Reducing the risk of hallux abducto valgus (bunion).
Dynamic arch support and efficient plantar loading through the foot.
Lateral ankle ligament protection.
When the peroneal muscles are weak or tight, there may be significant implications for foot and ankle function such as:
Gait
Weakness can lead to delayed eversion during gait and altered foot mechanics.
Postural control
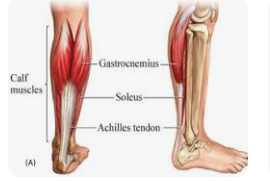
Tight or hyperactive peroneal muscles can alter the alignment of the subtalar/lower ankle joint and compensatory overuse of adjacent structures e.g. tibialis posterior.
Dynamic stability
Delayed peroneal activation reduces dynamic stability and impairs performance in activities that require rapid directional changes or single leg stance such as sports.
Injury risk
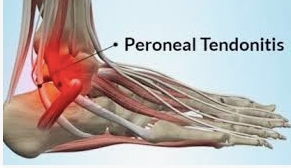
Weak peroneal muscles increase risk of lateral ankle sprains and tendon damage (peroneal tendinopathy).
Conditions involving the peroneal muscles
Peroneal tendonitis.
Partial tendon and muscle tears.
Peroneal tendon instability.
Chronic ankle instability.
Compression of the superficial peroneal or sural nerve.
Assessment of peroneal muscles
Gait
Peroneus longus resists ankle inversion (foot turning inwards) during initial contact, stabilising the arch in midstance and a small amount of plantar flexion during propulsion.
Where there is dysfunction, these phases of the gait cycle are affected, and even more so in dynamic activities.
Manual muscle testing
Resist the turning of the foot outwards (eversion). Peroneus brevis in neutral position and peroneus longus with foot pointed forwards (plantar flexion).
Proprioceptive and neuromuscular assessment
Single leg balance test: Static or dynamic.
Objective star excursion balance test: Reliable measure of a valid dynamic test. Single leg squat with the non-stance leg reaching to a point along one of eight lines at 45 degrees from each other.
Y-balance test: Modified version of SEBT with good inter-rater reliability. Use of anterior, posteromedial and posterolateral directions.
Other tests
Dynamic tests (hopping or lateral cutting on one leg).
MRI.
Ultrasound.
Electromyography.

Rehabilitation and management
We aim to train the peroneal muscles and improve the tissue tolerance to variations of load and position, generally increase strength and movement of the feet and ankles, and build on the ability to tolerate plyometrics and changes of direction required.
In acute injuries where the patient is unable to tolerate load, we focus on pain management and reducing inflammation. Ultrasound, acupuncture, bracing or taping can be used to reduce inflammation and stress on the peroneal tendons and allow early mobilisation.
Isometric/static exercises are early strengthening exercises that target the peroneal tendons without aggravating them.
Banded exercises are ideal for progressive resistance. When the patient can tolerate full weight-bearing activity, heel raises can be used with or without weight added.
There are a lot more exercises that can be added depending on the patient and sports specific rehabilitation using multi directional and high impact movements that mimic the demands of the sport or activity can be used. Examples include...
Single leg balance on Bosu.
Lateral jumping.
Running and turning.
Extracorporeal shockwave therapy has been shown to promote healing in chronic tendinopathies by stimulating collagen production and reducing pain. This has been successfully used by our team.
Orthotics could be used to offload peroneal strain or counter hindfoot varus.
If you would like to book an appointment with our team of experienced physiotherapists and sports massage therapists, call one of our friendly clinics:
Sheffield Physiotherapy: 0114 235 2727
Hope Physiotherapy: 01433 623 602